This is a summary of the study setup and most important findings of a scientific paper published in Journal of Wound Care (JWC) in September 2018. It is part of our “In a nutshell” series where we report the basics of all the scientific papers making up the Evidence for Woulgan, to make the findings more accessible.
Type of study:
This was an evaluation study conducted in a real-life clinical setting where the study treatment was compared with patients receiving standard of care (SC) from a database from the previous year. All patients were assessed by the same clinician (the author of the paper) and application of treatment were performed either by healthcare professionals or in some cases the patients themselves or their carer. The study was performed in a community setting.
- Evaluation study of 300 patients
- 150 patients treated with study treatment (Woulgan)
- 150 patients receiving SC, data from previous year (Control)
Wound types/patient characteristic:
Wounds of any aetiology deemed slow healing that met the inclusion criteria were recruited. Slow healing wounds were defined as wounds having less than 40% size reduction over 4 weeks. Wounds over 6 months old were not included as these wounds were referred to the hospital sector and thus was not assessible for recruitment. Patients self-presented to their GP and was then referred to the authors wound clinic for treatment.
Table 1: Patient and Wound parameters for study and control group
| Woulgan | Control | |
|---|---|---|
| Average age patients (years) | 57 | 52 |
| Average age wounds (months) | 2,5 | 2,3 |
| Average wound size (cm2) | 31,4 | 23,9 |
| Acute wounds (Post op, burns, trauma etc.) | 74 | 75 |
| Chronic/ulcer type wounds (DFU, LU, PU) | 76 | 75 |
Inclusion/exclusion criteria:
| Inclusion | Exclusion |
|---|---|
| Age over 5 years | Under 5 years |
| No infection | Diagnosis of infected wound |
| No antibiotics | Receiving antibiotics |
| Wounds with <40% size reduction over 4 weeks | Wounds with >40% size reduction over 4 weeks |
| Wounds deemed chronic (over 8 weeks old) | Wounds not being present for 8 weeks |
| Patient/carer who can follow written/verbal information | Patients/carer who cannot follow written/verbal information |
| Patient/carer giving verbal consent | Patient/carer declined verbal consent |
Treatment and application
Woulgan was applied at every dressing change twice weekly until healed or for maximum 8 weeks. Patients were continued on their pre-existing dressing regime, including offloading/compression for patients requiring this to minimise possible influence of changes in dressing regime. Woulgan was used as an adjunct therapy. Wounds were assessed at weeks: 0, 1, 2, 3, 4, 8, 12, 16, 20 and 24.
Tweet this: @woulgan doubled the healing rate for ulcer type wounds compared to standard care
Main findings
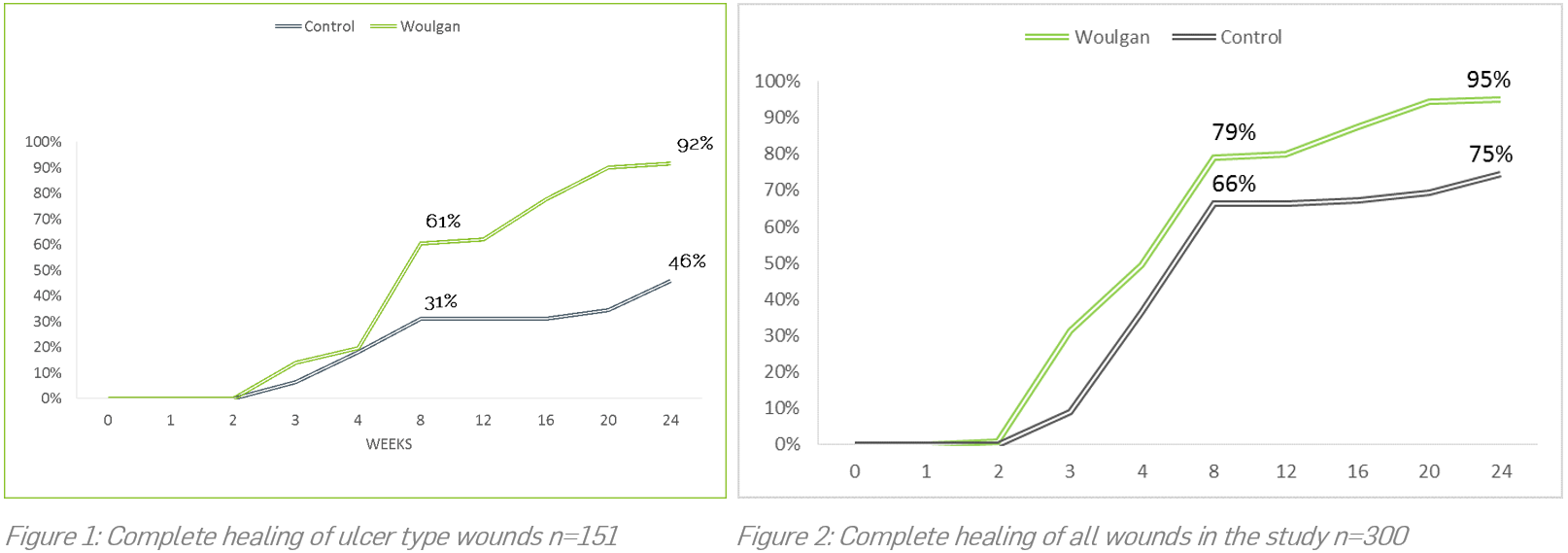
All the wounds treated with Woulgan responded to the therapy with a mean shorter healing time compared to the control group (Figure 2). However, the greatest impact was seen when splitting the slow healing acute wounds (trauma, burns, post op) with ulcer type wounds (DFU, VLU, ALU, PU). The cohort consisting of ulcer type wounds acknowledged as notoriously hard-to-heal had a significantly higher complete healing rate compared to control ulcers (Figure 1). The complete healing rate for Woulgan for ulcer type wounds were 61% at week 8 and 92% at week 24 compared to 31% and 46% for control.
- Double healing rates for Woulgan vs standard care
- 92% wounds completely healed with Woulgan
- 46% wounds completely healed with standard care
Conclusions and limitations
This study showed significant superior healing rates for Woulgan over standard care starting from 8 weeks up until week 24 from an initial 8 weeks treatment period. The complete healing rate at week 24 was 92% for ulcer type wounds treated with Woulgan compared to 46% for the control group, a doubling of the healing rate demonstrated for Woulgan. The control group and the Woulgan group were well matched and any differences was favouring the control group (Table 1). The study was carried out in a community setting which influenced the wound age (2,5 months average) at initiation as well as patient age (57 years average). Thus, the study demonstrates the major positive effects of escalating the standard care treatment to include Woulgan at an early timepoint post manifestation of the wound. The relatively low average age of the patients might have contributed positively for the high healing rates as old age in general negatively affect healing. However, there were no significant age differences between the control and study group, thus the benefits of adding Woulgan as an adjunct therapy to standard care is confirmed with this study.